The Shroud of Turin: Beyond Science?
Posted on 24 April 2017, 9:45
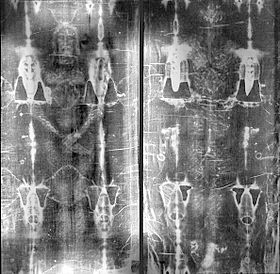
While watching the History Channels Easter special on the Shroud of Turin (The Face of Jesus Uncovered?), I was in awe of the capabilities of science and computer technology; however, I was also reminded of their limitations. The scientists studying the shroud (below) concluded that it is not a painting or some creative fabrication. They can tell what it isnt but not what it is.
I have read quite a bit about the shroud and have seen at least a half dozen other documentaries on the relic that many believe covered the crucified body of Jesus of Nazareth two-thousand years ago, but this one went beyond all others, moving me from being very skeptical to just somewhat skeptical as to whether the shroud is in fact the burial cloth of Jesus. Prior to this documentary, I was about a 20 percent believer (80 percent doubter) in the authenticity of the shroud, but I am now an 80 percent believer. My 20 percent doubt is divided between it being the image of someone other than Jesus and some form of fraud that goes beyond modern science.
Like so many others, I pretty much dismissed the shroud as being authentic after the carbon-14 tests in 1988 dated it to around the fourteenth century. My belief factor was then down to about two percent. I began reconsidering it a few years later when it was pointed out that the carbon testing was from a small edge of the shroud that was contaminated from frequent handling and from repairs due to fire damage 700 or so years ago. Moreover, it was reported that pollen from an artichoke plant native to the Jerusalem area was found embedded in the fibers.
What the scientists in this most recent documentary pointed out that I had not heard before was that a 3-D image analyzer revealed that there are contours in the image distortions resulting from the cloth being draped over a body thus strongly suggesting that the shroud was in fact wrapped around a human body. Such contours are not found in paintings or other art work, making it highly unlikely that it was an artistic endeavor by Leonardo da Vinci or some other artist from that era, as so many have come to believe. And while the image on the shroud appears to be a man much older than 33, the age at which Jesus is said to have been put to death, a computer graphics artist was able to eliminate the contours and turn the two-dimensional image on the shroud into a three-dimensional figure, the result being a much younger man, one of perhaps 33.
Add in the fact that the numerous blood stains on the shroud were subjected to testing and found to be real blood with DNA indicating an ethnicity from the area around Jerusalem. On top of that, the numerous blood stains on the shroud are consistent with wounds resulting from both scourging and crucifixion, including a crown of thorns. While there is evidence that many others were crucified in Jesus time, indications are that scourging was not part of the execution process, and it seems very unlikely that a crown of thorns would have been placed on the victim. To put it another way, the wounds on the shroud image are totally consistent with the biblical account of the crucifixion of Jesus and not consistent with what is known about other crucifixions.
Another interesting fact mentioned in the latest documentary has to do with the sudarium, a face cloth that is said (John 20:6-7) to have been draped over Jesus face before the shroud was placed over him. The sudarium has long been preserved in a chapel in Oviedo, Spain. Forensic testing has lined up the blood on the sudarium with the blood on the shroud. While carbon-14 testing has dated the sudarium to around 700 AD, the history of this particular sudarium goes back to approximately 570 AD, and the laboratory noted that later oil contamination could have resulted in faulty testing.
Those involved in studying the shroud cannot offer a scientific explanation as to how the image was imprinted on the 14-foot long linen. It was explained that diffused light would not make such an imprint. The bottom line is that it is presently beyond science. Of course, the religious explanation is that it resulted from some supernatural burst of energy that is called the resurrection.
While the orthodox Christian belief is that the physical body of Jesus left the tomb and that he visited with his disciples before ascending to heaven, the teachings that have come to us in more recent times from the spirit world through credible mediums tell it differently. I believe the explanation given to Johannes Greber (below) by a seemingly advanced spirit, through the mediumship of a young man, offers the more rational view. As you are able to convert matter into steam with the aid of high temperatures and even to cause this steam to become invisible to the human eye, so also is the spirit-world able to dissolve matter completely, Greber, a Catholic priest turned psychical researcher, was informed. It too makes use of hot power-currents, by means of which it converts matter into an od-like, etherealized form. For, as I have explained to you, all matter is nothing but corporealized od which can be dissolved into spiritual od.
Od was the name given by German chemist Baron Karl von Reichenbach (1788-1869) to an energy that he discovered existing among sensitive people people with clairvoyant, clairaudient, and clairsentient abilities. It is said to be a life principle that permeates and connects all living things and has been likened to the prana of the ancient Hindus, the chi of the Chinese, the astral light of the Kabbalists, the vis medicatrix naturae of Hippocrates, the magnetic fluid of Mesmer, the orgone energy of Reich, and the ectoplasm of mediums. It is apparently present in all humans, although those with mediumistic ability have it in greater quantities, though not necessarily in greater quality.
Indications are that the misty vapors often observed leaving the body of a dying person are od. It acts as sort of a glue in bonding the physical body with the spirit body, and the more materialistic the person the denser the od and the more difficult the separation.
Not even of Christ was the natural body raised, Greber was further informed. Like the physical bodies of all mortals it had been created from the od of the earth and like them it returned to earth, with this exception, that it was not redissolved into terrestrial od by way of decay, but by dematerialization effected by the spirit-world. It was further explained that when Jesus appeared to his disciples after his death, his odic body materialized, and when he departed the odic body dematerialized.
As I see it, the survival or resurrection message is not affected one iota by accepting that the physical body of Jesus dematerialized rather than believing that it went to heaven. Im at 99.9 percent on that.
Michael Tymn is the author of The Afterlife Revealed: What Happens After We Die, Resurrecting Leonora Piper: How Science Discovered the Afterlife, and Dead Men Talking: Afterlife Communication from World War I.
Next blog post: May 8
Read comments or post one of your own
|

